
(Credit: Mark Winfrey/Shutterstock)
LOS ANGELES — In the quiet corners of American neighborhoods, a critical healthcare crisis is unfolding — one prescription at a time. Pharmacies, once as abundant as corner grocery stores, are disappearing at an unprecedented rate, leaving communities — especially those most vulnerable — struggling to access essential health services.
A study published in the journal Health Affairs reveals a startling transformation of the pharmacy landscape: nearly one in three U.S. retail pharmacies has closed since 2010, with an accelerating decline that threatens to reshape healthcare accessibility across the nation.
“At the same time many states are making efforts to expand the scope of pharmacy services beyond dispensing drugs to include the provision of preventive and emergency care, we found that there are—for the first time for at least a decade—fewer pharmacies available to provide them,” says Dr. Dima Mazen Qato, senior author of the study and an associate professor at the USC Mann School of Pharmacy and Pharmaceutical Sciences, in a university release.
The review, conducted by researchers from USC and UC Berkeley, paints a stark portrait of pharmacy accessibility. Between 2018 and 2021, pharmacy closures swept across 41 states, impacting a staggering 91.6 million people. The most devastating losses were concentrated in predominantly Black and Latino neighborhoods, where closure rates reached 37.5% and 35.6%, respectively, compared to 27.7% in predominantly White communities.
Independent pharmacies bore the brunt of these closures, facing more than double the risk of shutting down compared to chain stores. These local businesses, often the lifeline of underserved communities, found themselves systematically squeezed out of the market.
“Our findings suggest that closures may widen health disparities in access to prescription and other essential pharmacy services,” explains Jenny Guadamuz, the study’s first author and an assistant professor at UC Berkeley’s School of Public Health. “Without safeguarding pharmacies in marginalized neighborhoods, expanding health care services at pharmacies may enhance convenience for more affluent populations while failing to address the health needs of communities disproportionately affected by pharmacy closures, particularly Black and Brown populations in low-income urban areas.”
The root of the problem lies in complex market dynamics. Pharmacy benefit managers (PBMs) — companies that negotiate prescription drug benefits — have increasingly steered patients toward preferred networks, often excluding independent pharmacies. Recent mergers between large pharmacy chains and PBMs have further exacerbated this trend, creating an environment where smaller pharmacies struggle to survive.
The consequences extend far beyond mere inconvenience. Pharmacies are critical healthcare access points, offering services that go well beyond dispensing medications. Vaccinations, HIV prevention medications, contraceptive prescriptions, and treatments for opioid use disorder are just a few of the essential services now at risk of becoming less accessible.
The researchers propose several policy interventions to address this crisis:
- Mandate Medicare and Medicaid plans to provide preferred status to pharmacies at high risk of closure
- Require PBMs to create networks that don’t disproportionately favor large chain pharmacies
- Increase reimbursement rates for pharmacies serving vulnerable communities
“Federal, state and local policies and programs should consider targeted strategies, including increases in Medicare Part D and Medicaid pharmacy reimbursement rates, to protect critical access to pharmacies most at-risk for closure,” Dr. Qato emphasizes.
The vanishing of local pharmacies is more than an economic trend — the research team says it’s a public health emergency that demands immediate attention. In the delicate ecosystem of community healthcare, every closed pharmacy represents not just a business lost, but potential lives impacted.
Paper Summary
Methodology
The researchers used a comprehensive database from the National Council for Prescription Drug Programs, tracking every retail pharmacy in the United States from 2010 to 2021. They cross-referenced this information with census data, examining pharmacy locations, neighborhood characteristics, and closure rates.
The team categorized pharmacies by type (chain, independent, or other) and neighborhood demographics, including racial composition, income levels, and insurance coverage. This allowed them to analyze how different factors might influence pharmacy survival.
Key Results
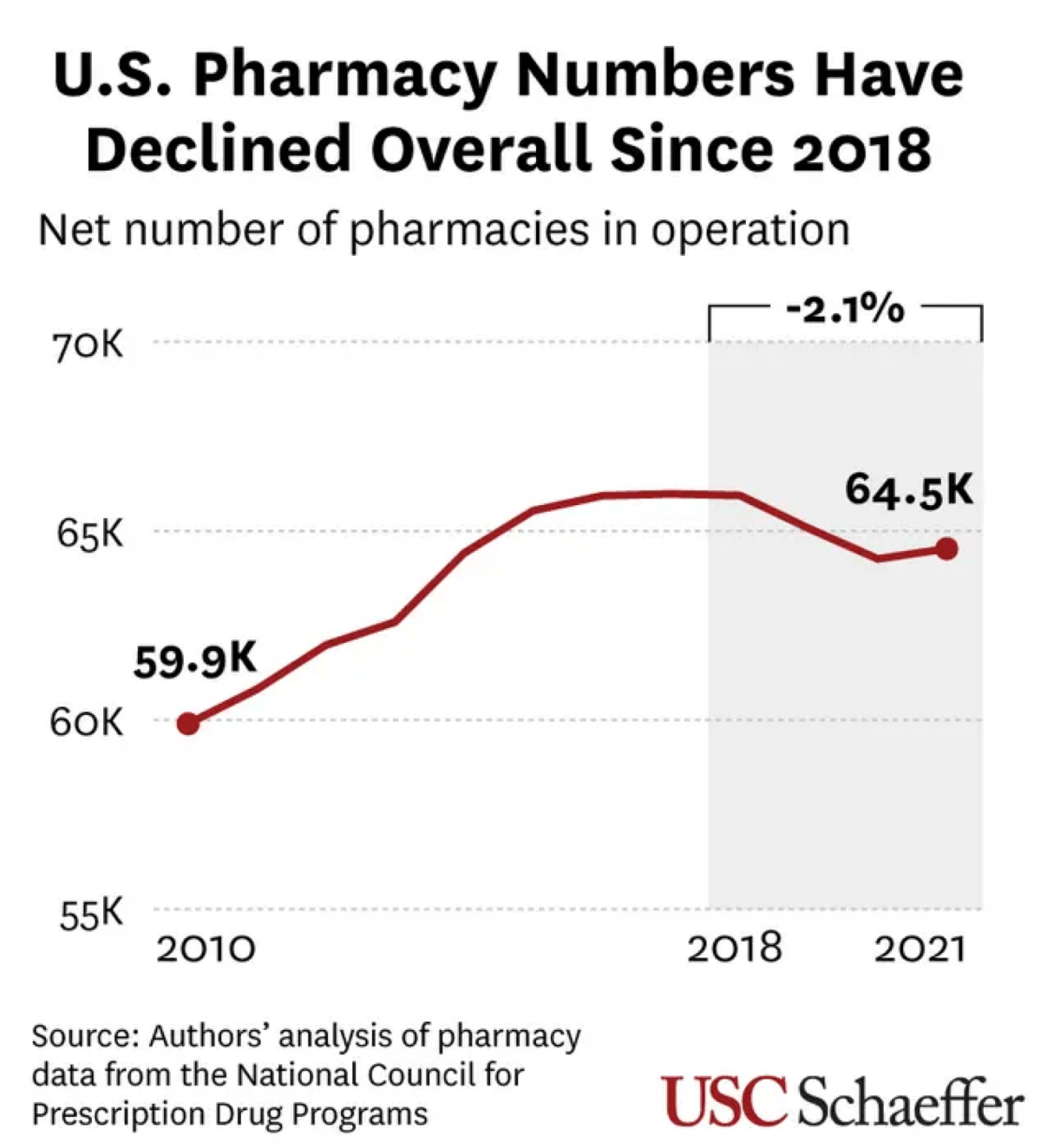
Out of 88,930 pharmacies examined, 26,145 closed during the study period. While the total number of pharmacies initially grew between 2010 and 2017, a significant decline began in 2018.
Geographically, the closures were not uniform. Some states, like North Dakota and Arizona, saw pharmacy closure rates below 20%, while others, like New York and West Virginia, experienced rates above 35%. By 2021, 41 states had experienced net losses in pharmacy numbers.
Study Limitations
The researchers acknowledged that they couldn’t track the exact volume of prescriptions filled at each pharmacy or fully analyze the complex dynamics of pharmacy benefit managers’ networks. The data also couldn’t account for potential impacts from the COVID-19 pandemic or trends in mail-order pharmacy usage.
Discussion & Takeaways
The study highlights a critical healthcare accessibility issue. Independent pharmacies, which are more likely to serve marginalized communities, are disappearing at an alarming rate. This trend could exacerbate existing racial and ethnic disparities in healthcare access.
The researchers propose several policy recommendations:
- Mandate the inclusion of independent pharmacies in preferred pharmacy networks
- Increase Medicaid reimbursement rates for at-risk pharmacies
- Create targeted strategies to protect pharmacies in vulnerable neighborhoods
Funding & Disclosures
The research was supported by a grant from the National Institute on Aging, part of the National Institutes of Health. The funding organization had no role in the study’s design, data analysis, or manuscript preparation.







